Idiopathic Intracranial Hypertension
(Pseudotumor Cerebri)
December 17, 2009, updated February 2, 2010
Chief Complaint: Headaches and transient double vision for 6 months
History of Present Illness:
A 31-year-old obese female presented to her eye doctor with a history of headaches and transient visual obscurations for six months. She also reported a ringing sound in her ears for the past year that was synchronous with her pulse. On exam, she was noted to have bilateral optic disc edema. An MRI scan was performed and was normal except for an empty sella. The MR venogram was normal with no evidence of sinus thrombosis. She was diagnosed with idiopathic intracranial hypertension and referred to a neurologist for further workup and management. The neurologist performed a lumbar puncture which showed an elevated opening pressure of 50 cm H2O. The patient was started on acetazolamide (Diamox®) 500 mg twice a day and encouraged to lose weight.
The patient continued to have severe headaches after the lumbar puncture. One month later, she returned to her eye doctor for visual field testing. Humphrey perimetry was performed, and showed a mean deviation of -20.85 in the right eye with enlargement of the blind spot and a dense nasal field defect. In the left eye, the mean deviation was -20.35 and also showed enlargement of the blind spot and a dense nasal field defect. A repeat lumbar puncture was performed, which again showed an elevated opening pressure of 50-56 cm H2O. Her Diamox dosage was increased to 500 mg three times daily and she was subsequently was referred to the Neuro-ophthalmology Service at UIHC for further evaluation and management.
Past Ocular History: Prior eye examination at UIHC in 2000 was normal.
Past Medical History: Obesity and Depression.
Medications: Acetazolamide (Diamox®) 1500 mg daily, citalopram hydrobromide (Celexa®)
Family History: Non-contributory
Social History: Non-smoker, denies alcohol use
Review of Systems: She reports significant weight fluctuations over the last several months.
Physical Exam:
- Visual Acuity
- OD-- 20/20
- OS-- 20/50
- Extraocular motility: full OU, without diplopia
- Pupils: 5 mm in the dark and 2 mm in the light; no relative afferent pupillary defect.
- Intra-ocular pressure: 11 mmHg OD, 16 mmHg OS
- Color vision testing normal in each eye.
- She had normal cranial nerve V and VII function bilaterally.
- External and slit lamp exam normal
- The patient had grade two papilledema. The macula, vessels and periphery in each eye were normal. (see figure 1)
 |  |
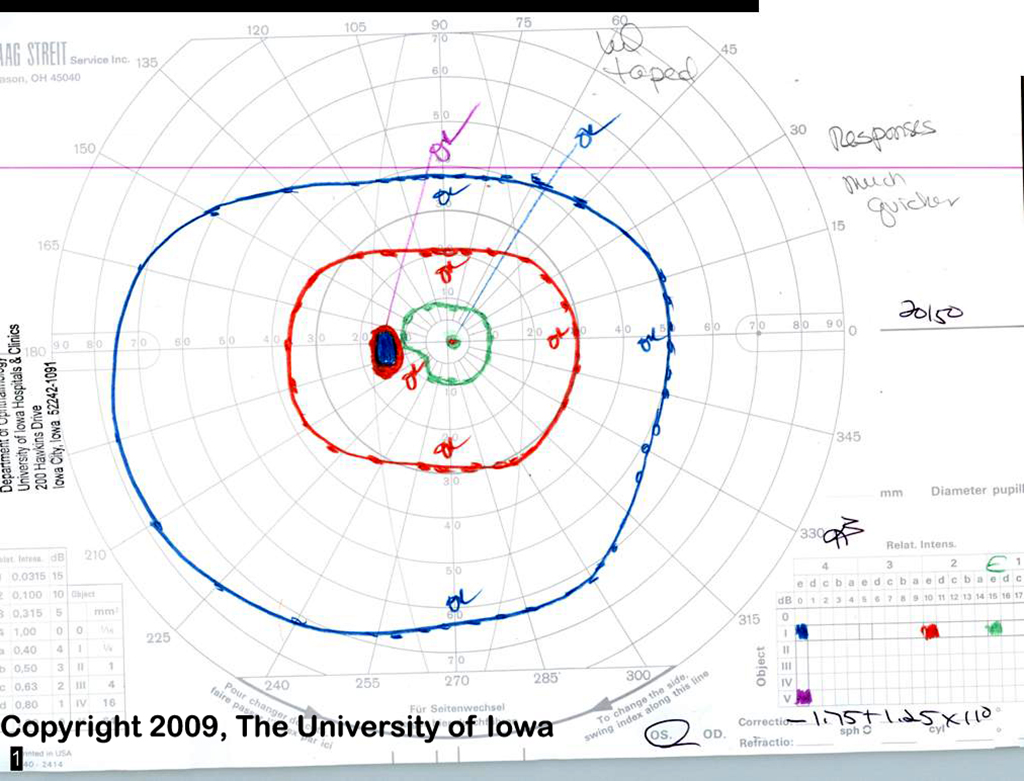 |  |
| The right eye field shows a markedly enlarged blind spot and some nasal constriction. The left eye field shoes a small paracentral scotoma to the 11e and 12e isopter, but full peripheral field. The patient reported having transient visual obscurations during testing of her left eye. | |
 |
Course
The patient's dose of Diamox was increased to 2 gm daily, given that she had papilledema, persistent headaches, transient visual obscurations and pulse synchronous tinnitus. When she returned two weeks later, she felt better. She had lost 5.5 pounds and her headaches had resolved. Her visual acuity was 20/20 OD and 20/25 OS and ophthalmoscopy showed residual grade I-II disc edema. Her Goldmann visual field had improved. She was kept on the same dose and returned for follow up, 2 months later.
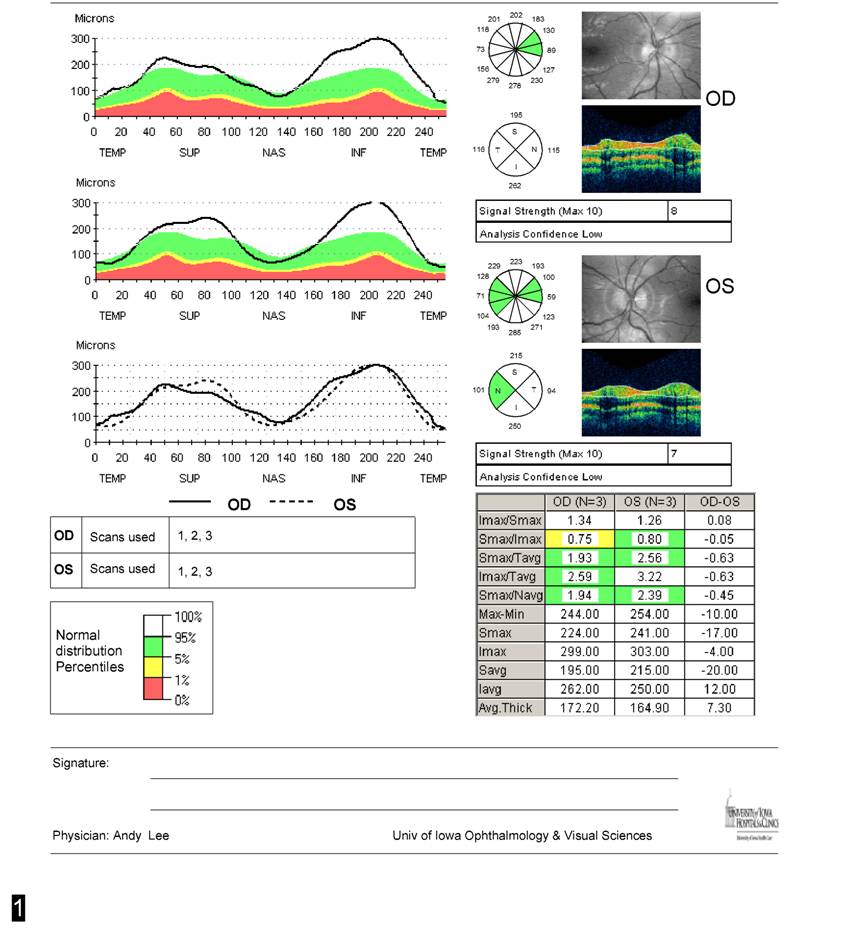
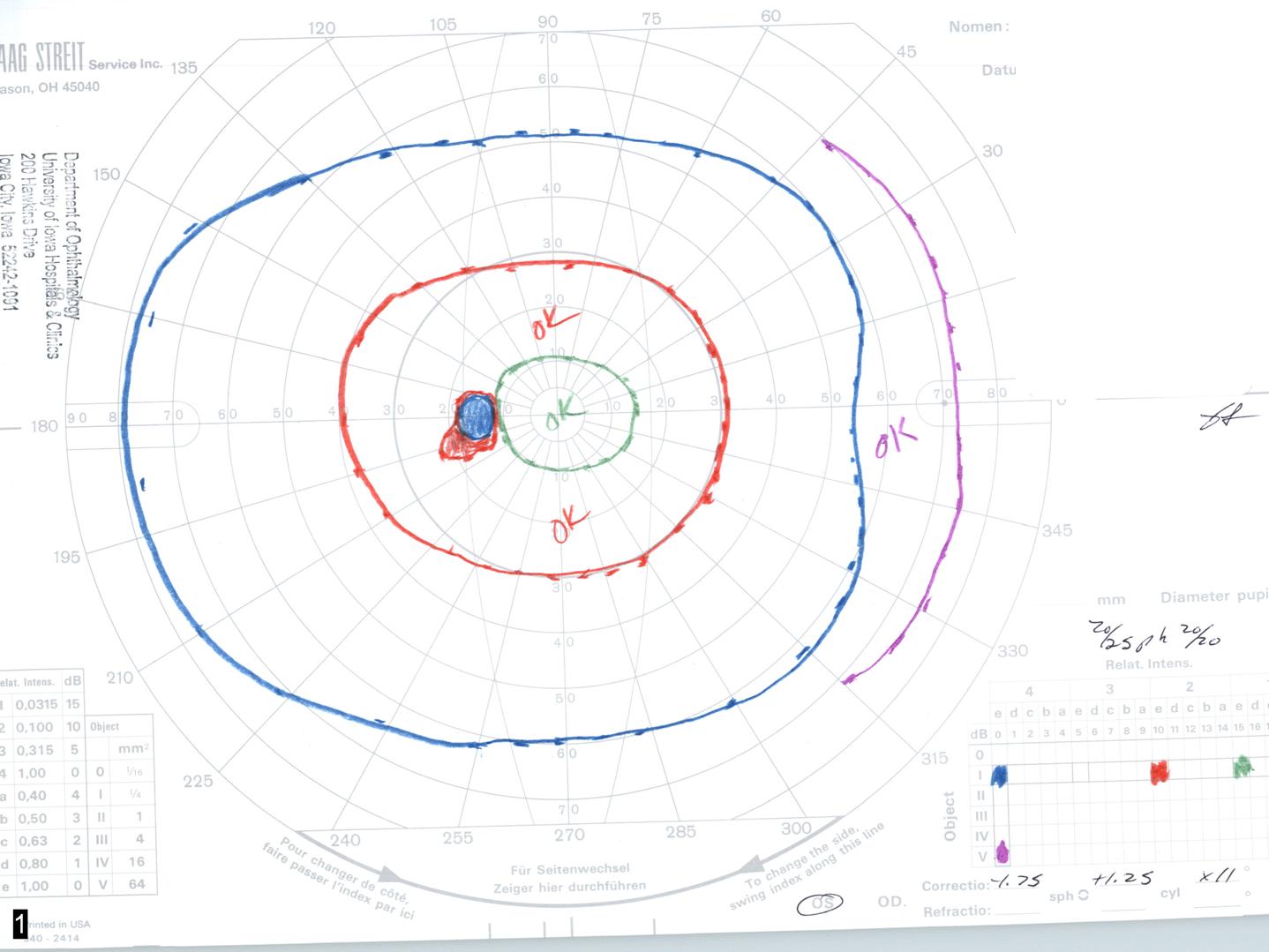
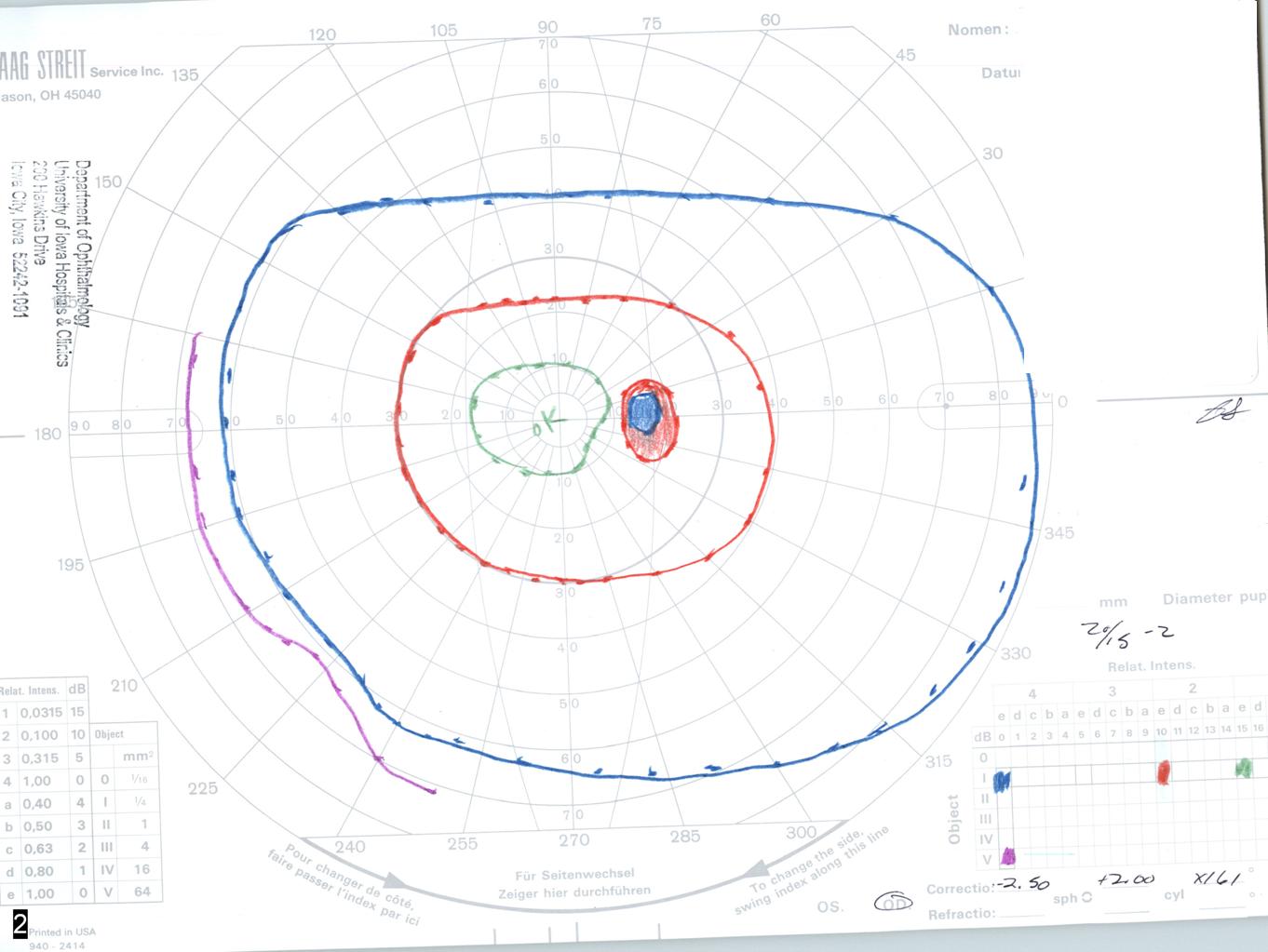
At her follow up appointment she reported only three headaches since her last exam. She had lost an additional 4.5 pounds for a total of 10 pounds of weight loss. Goldmann visual field showed a slight enlargement of the blind spot on the left greater than the right. The rest of the field was full. Her visual acuity was 20/15 OD and 20/25 OS and ophthalmoscopy showed grade I optic disc edema. (see figures 3 and 4)
She has since been doing well and her Diamox was tapered off without further complications. She continues to be followed by the neuro-ophthalmology clinic.
 |  |
 |  |
Discussion
Idiopathic Intracranial Hypertension (IIH) is a condition in which the cerebrospinal fluid (CSF) is under high pressure in the absence of an intracranial mass, venous sinus thrombosis or other primary cause (see differential diagnosis). It is also known as pseudotumor cerebri because patients present with signs and symptoms of a brain tumor without a brain tumor being present.
Pathophysiology
In IIH, there is no structural obstruction to the circulation of CSF. It is believed that the problem lies in defective reabsorption of CSF either at the level of the arachnoid granulations or along cranial and spinal nerve root sheaths. There is no evidence for excessive CSF production.
There is a female preponderance for this disease, and the peak age of onset is in the third decade of life. It is common for affected patients to be obese, and weight loss is an important part of treatment. IIH symptoms often start or worsen during a period of weight gain and resolve with 5-10% total weight loss. The disease is rare in thin men. This has led some researchers to look for an association with hormonal changes within the body, but to date no consistent associations have been found. The disease has been associated with withdrawal from steroids, and with the use of exogenous substances like vitamin A, tetracyclines, and oral contraceptives.
Although no associated conditions besides recent weight gain are usually found, many conditions have been linked to high intracranial pressure. Any disorder that blocks the flow of spinal fluid between the brain and the jugular venous system can cause raised pressure. For example, scarring of the arachnoid granulations by meningitis can cause raised intracranial pressure. Similarly, blood clots in the veins draining the brain can cause increased intracranial pressure. These conditions can mimic IIH.
Symptoms and Signs
IIH presents with symptoms and signs of elevated intracranial pressure. Headache is the most common symptom. The headache may be aggravated by changes in position. There may be a ringing or a "whooshing" sound in the ear synchronous with the patients pulse. A patient may experience double vision. Momentary loss of vision known as "transient obscurations of vision" are common; they may occur in one or both eyes and usually last seconds but rarely longer than one minute. Other visual symptoms are dimming of vision, or loss of peripheral vision in one or both eyes. The visual loss may be mild to severe. If severe and untreated, the disease can result in permanent vision loss.
A prospective study conducted by Wall and George demonstrated the following incidence of symptoms
- headache (94%)
- transient visual obscurations or blurring (68%)
- pulse synchronous tinnitus or "whooshing noise" in the ear (58%)
- pain behind the eye (44%)
- double vision (38%)
- visual loss (30%)
Over 90% of patients in this study had visual loss documented by perimetry (Wall and George, 1991).
On examination, papilledema (bilateral optic disc edema) is nearly always present. This may be accompanied by a serous retinal detachment and choroidal folds if the intracranial pressure is excessively high. (see images of Grades I-V papilledema)
.jpg) | .jpg) | .jpg) | .jpg) | |
Diagnosis
First, imaging studies of the patient's head (via magnetic resonance imaging or computed tomography) must be normal except for the signs of raised intracranial pressure (empty sella, flattened globes, collapsed lateral sinus). Next, the cerebrospinal fluid pressure is measured by a lumbar puncture and the pressure must be elevated. The lumbar puncture should be performed with the patient in a supine position for most accurate measurement of the intracranial pressure. Laboratory studies on the cerebrospinal fluid must be normal. All of the above criteria (the Modified Dandy Criteria, see table) must be met in order to diagnose IIH.
|
Treatment
A variety of treatments for IIH have been proposed and there is much anecdotal evidence for these treatments. There is no evidence-based data currently available but an NIH sponsored clinical treatment trial is beginning in 2009. Patients with no visual loss or mild visual loss are treated medically.
Weight loss is an important part of treatment and is always recommended. Most patients improve after losing 5-10% of their total body weight. It appears that in addition to weight reduction, sodium restriction is also a useful adjunct. We recommend that patients lose about one pound a week for several months and then maintain the weight loss. The mechanism of the beneficial effect of weight loss on this disease is unclear but there are parallels with the beneficial effect of weight loss and sodium restriction for treatment of essential hypertension.
For patients requiring medical therapy, acetazolamide (Diamox®) is the most commonly used medication. It is relatively safe but nearly all patients experience the side effect of paresthesias, or numbness and tingling in the extremities. Patients also report an alteration in taste such that carbonated soft drinks taste metallic. Less commonly, kidney stones can occur. Another diuretic commonly used that appears to be effective in some patients is furosemide (Lasix®). Topiramate (Topamax®) is used for migraine prophylaxis and has been found to be effective in the treatment of headaches associated with IIH.
Intractable headache or progression of visual loss despite maximal medical treatment requires surgical therapy. The primary surgical options are optic nerve sheath fenestration or a CSF diversion procedure (shunt). Optic nerve sheath fenestration involves the creation of a window in the sheath-like covering of the optic nerve. This creates an outlet for escape of cerebrospinal fluid and alleviates the direct pressure on the optic nerve. Later, the area around the nerve within the nerve sheath scars down further protecting the optic disc from damage.
Placement of a shunt (lumboperitoneal or ventriculoperitoneal) is another surgical treatment option. The device diverts cerebrospinal fluid to the abdomen or into the jugular vein (ventriculojugular). Both types of surgeries have their own risks and benefits and unfortunately about 50% of shunts fail at some point.
.jpg) |
Diagnosis: Idiopathic Intracranial Hypertension (Pseudotumor cerebri)
Differential Diagnosis
Highly Likely
- Decrease flow through arachnoid granulations
- Scarring from previous inflammation (meningitis, sequel to subarachnoid hemorrhage)
- Obstruction to venous drainage
- Venous sinus thrombosis
- Hypercoagulable states
- Contiguous infection
- Bilateral radial neck dissections
- Superior vena cava syndrome
- Increased right heart pressure
- Endocrine Disorders
- Addison's disease
- Hypoparathyroidism
- Obesity
- Steroid withdrawal
- Nutritional Disorders
- Hypervitaminosis A (vitamin, liver, or isotretinoin intake)
- Hyperalimentation in deprivation dwarfism
- Arteriovenous malformations
- Obstructive Sleep Apnea
Probable causes
- Anabolic steroids
- Kepone
- Ketoprofen or Indomethacin
- Systemic Lupus erythematous
- Thyroid replacement therapy in hypothyroid children
- Uremia
Possible causes
- Amiodarone
- Diphenylhydantoin
- Iron-deficiency anemia
- Lithium carbonate
- Nalidixic acid
- Sarcoidosis
- Sulfa antibiotics
EPIDEMIOLOGY
| SIGNS
|
SYMPTOMS
| TREATMENT
|
No comments:
Post a Comment